Healthy City – Healthy Settings Planning.
Between disciplinary contributions and interdisciplinarity
Maria Chiara Torricelli

Keywords:
Healthy Cities, Built Environment, Place-Based Approach, Research-Based Planning
Abstract:
The topic of health in the design of urban and building spaces represents an emerging problem within the scope of the larger problems of sustainable, environmental and social development, and respect for cultures and people. This article raises some questions about the interdisciplinary nature of this topic, the aspects it takes on at different scales and in different contexts, and the specific role of urban design and construction. Raising these questions allows us to contextualise the problems and understand their complexity and the responsibilities in addressing them professionally and in architectural research. To do this, reference is made to international programmes on this subject, the positions assumed by researchers and operators, and projects recognised as exemplary in terms of attention to people’s health and well-being.
Introduction
Healthy Place, Healthy City is a topic that deals with the relationship between the spaces in which we live and people's health and well-being, from a multitude of aspects and with reference to different contexts. As stated at the International Conference Healthy Cities held in Belfast in October 2018, health and well-being in the settlements we live in imply conditions of equality, peace and security, and the prospect of sustainable development 1 . Within policies, societies, economies and cultures there are responsibilities and expertise specific to research and different professions. Health, as it relates to the environment, assumes different importance in countries located in the north and south of the world with respect to the vulnerability of groups of people, conditions of marginalisation and access to socio-healthcare services, and the fragility of the territories. Health is place-based (Lawrence, 2015), that is it depends on factors of the physical and social context and entails the involvement of the community and region; but at the same time, it is also the result of “global” impacts and must be protected at different levels2 , with a commitment that involves different disciplines, different players and different people.
Healthy Setting, Healthy City. What does this mean?
The terms Healthy Setting and Healthy City were coined by the World Health Organization (WHO) between 1980 and 19863 and indicate a continuous process of creating and improving the physical-environmental and social conditions and expanding the resources of a community in order to enable people to support each other in all aspects of life and in the full development of their potential4 . In the foreground are cities, now occupied by over 55% of the global population and capable of promoting or damaging health and the quality of life. The WHO Healthy Settings and Healthy Cities programmes were launched at the same time as the Brundtland Report (WCED, 1987) on sustainable development, but they are rooted in the very establishment of the WHO5 . In 1986, the WHO specifically intended to propose a settings-based, holistic and interdisciplinary approach aimed at developing integrated actions for different risk factors, participation and the empowerment of communities, intersectoral partnerships and fairness. Projects and programmes are endorsed in the different regional groupings into which the WHO divides the world, and are organised according to settings: Cities, Villages, Municipalities and Communities, Schools, Workplaces, Markets, Residences, Islands, Hospitals, Prisons, Universities, Life of the Elderly6 . The first programmes concerned cities in developed countries such as Canada, the United States, Australia and different nations in Europe, and thereafter, in the mid-Nineties, programmes were launched in emerging and developing countries. The Healthy Cities network now includes over 1000 cities worldwide. In the 2000s developing countries saw the launch of the Healthy Villages programmes, which aim to promote health in rural areas and focus on the specific problems of these areas, such as: the fight against infectious diseases and neonatal mortality, access to services and safety.
The topic of health and cities was also confirmed in the objectives of the UN’s 2030 Agenda for Sustainable Development, the Sustainable Development Goals (SDGs)7 .
A global and local set of problems
Like all topics linked to the sustainability of development, and in particular those more directly linked to people, communities and settlements, the topic of Healthy Cities and Healthy Settings is highly contextualised. The city and rural village levels are identified as the appropriate dimensions for a community, with reference to the role of governance, albeit with different roles as regards large conurbations, regional cities, and rural cities or centres. For villages in particular, the topic of health cannot overlook the relationship with the city. Healthy City issues in large cities concern, as a priority, aspects of environmental impact that damage human health, for example aspects that contribute to the Disability-Adjusted Life Years (DALY) indicator8 and that in cities are largely caused by mobility and industries. Factors such as ground and water pollution and the destruction of biodiversity influence health in rural areas too. These are environmental problems of regional or local significance. Some environmental aspects of global significance can in any case also directly or indirectly influence the health of individuals: the effects of global warming and the reduction of the ozone layer affect the elderly and children in particular, and increase the vulnerability of some regions (fires, floods, landslides); the scarcity of energy resources increases the cost and affects the poor. Social factors that impact health are regional/local in nature: access to the network of services, assistance for the weakest groups in the population, prevention, and healthcare education. The importance of healthy lifestyles for health has led, in particular in the programmes of countries in the north of the world, to issues such as “how do we live” and what habits do we form being addressed, also and particularly in relation to the management of places. What's the food like in cities? Where can one do sport, walk, play, and meet up?
The programmes
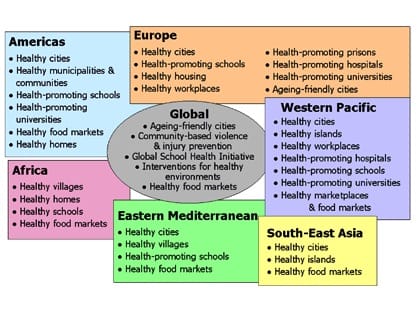
The WHO programmes cover different topics and contexts (fig. 1) in which the emerging problems are not the same, for example in city programmes the size of the resident population has a significant impact. Europe has been a pioneer on the topic of Healthy Cities (Hancock 1986, De Leeuw 2001), building a network as early as 1988, which is now divided into 100 “torchbearer” cities and around 30 national networks. The focus in these European cities is mainly on socio-healthcare projects aimed at population groups and on promoting an active life with interventions on urban green areas, pedestrian areas and cycle paths, and the issue of transport (WHO EURO 2013). The control of air, ground and water pollution, linked to control of the use of non-renewable energies and toxic and polluting materials, in Europe is governed by a complex and evolved system of legislation and control at EU and national level. Integration between these actions: services, the urban environment, atmosphere and biosphere, in relation to human health, is however an important matter to be tackled in Europe too (Valera Sosa, 2017a-b). (Fig.1)
In China, much emphasis has recently been placed on the health of cities after years of attempting to regulate air and water pollution with legislative measures and standards, and with the eco-cities programmes promoted as early as the mid-80s (Williams, 2017). In 2016, the People's Republic approved the Healthy China 2030 Planning Outline, and in 2017 Shanghai launched the Shanghai Healthy 2030 Plan which covers extensive action, from air, water and ground pollution to territorial and district health services, healthcare reform for residents and workers, health education, the protection of weak categories, up to the promotion of lifestyles that include physical activity and proper nutrition10 (Xiaodong 2017).
In Africa, the WHO Healthy Cities network, together with programmes like the Urban Health Initiative, prioritises air, ground and water pollution, urban and building hygiene and the improvement of health services in capital cities with a rapidly growing urban population living in slums. In Accra, the capital of Ghana, Ghana Health Services, with the support of the WHO, implemented a programme that has been in place since 2010 to train experts to monitor pollution, as well as healthcare service planners and physicians, along with building hygiene, waste management, road safety and urban green area programmes11 . More so than in other regions, in Africa Healthy Villages programmes are in place, and the WHO has developed a guide for rural villages (Howard et al.2002; WHO 2002) aimed at settlements of a certain size and with differentiated activities, whether these villages have an independent administration or are part of vast urban or regional areas. The guide covers hygiene education, health promotion and the reduction of the environmental impact, placed-related health, hygienic infrastructures (water, sewerages, waste), urban and building hygiene, and health services. Healthy Villages programmes are also active in South East Asia and in the Southern and Eastern Mediterranean. They involve contexts in which villages and the countryside, where a large part of the population still lives, undergo profound transformations due to the urbanisation processes underway, which can sometimes result in the incorporation of villages into the urban expansion, or their further marginalisation from basic services.
As regards the problem of health in the rapid urbanisation process, China is also addressing the problem of poverty and the marginalisation of the countryside where over 40% of the population still live, mainly the elderly. Between 2008 and 2015 a Healthy Villages project was developed following the WHO guidelines and supported by the World Bank12 . The priorities are: health education and hygiene education with regard to food, locations and the village, and basic health services. The programmes are now part of a process to develop rural provinces which China is focusing on in order to reduce inequalities between the city and the countryside, in particular promoting investments in redevelopment and tourism in historical villages, with the government’s recent launch of the National Strategic Plan for Rural Vitalisation (Williams, 2018).
In emerging and developed countries, rural villages can be not only a problem but also a resource to promote health, leveraging the desire to go back to living close to nature. This does not circumvent issues regarding access to the network of services and protection against natural disasters. Returning to Italy, for example, the topic of health in what are referred to as the “internal areas” and the islands is still topical due to the lack of territorial and emergency services (Barca et al. 2014) and the risks of natural disasters. This is why innovative experimental models for managing services aimed at the elderly, chronically ill patients and foreigners (visitors and immigrants) are promoted for these areas, such as: telemedicine, empowerment programmes, “Health Points” and the distribution of medicines.
Finally, also at the scale of buildings for the community, there are international and national programmes aimed at promoting health according to an integrated space-organisation vision (place-setting). Here we need only recall the establishment in 2007, with the support of WHO/Europe, of the international network Health promoting Hospitals and Health Services (Whitehead, 2004) and the different initiatives aimed at promoting healthy and sustainable hospitals (Wilburn et al. 2009). As regards housing, the WHO (2018) has recently developed a guide that addresses the topic of housing in relation to health, urban growth, the ageing of the population and climate change. In schools, the European Schools for Health network promotes good practices in school design, but many international and national investigations report conditions of bad indoor13 air quality, structural insecurity, and inadequate environmental comfort and usability (Stewart-Brown 2006). The WHO Healthy Schools reports the fact that, although the network is the most extensive and the second to be launched, the scarcity of national and local financing makes it difficult to implement intervention programmes14 .
The health-conscious architect
In Europe, from 1750, relationships between architecture and society started to radically transform, and gradually over the course of the 19th century it became clear that hygiene in housing was not enough to create sanitary conditions and the urban environment as a whole had to be tackled. But it was at the end of the 20th century that space was recognised as having role in the protection and promotion of the physical and mental health of people. Theories and experiences of urban and architectural design were developed along this trajectory, placing the focus on health and the well-being of people, supported by analytical studies and contributions from other professions. The design responsibilities and expertise that are now required as a priority to address this problem cannot be summarised in a few lines, and I shall limit myself to highlighting some aspects which I deem to be influential references.
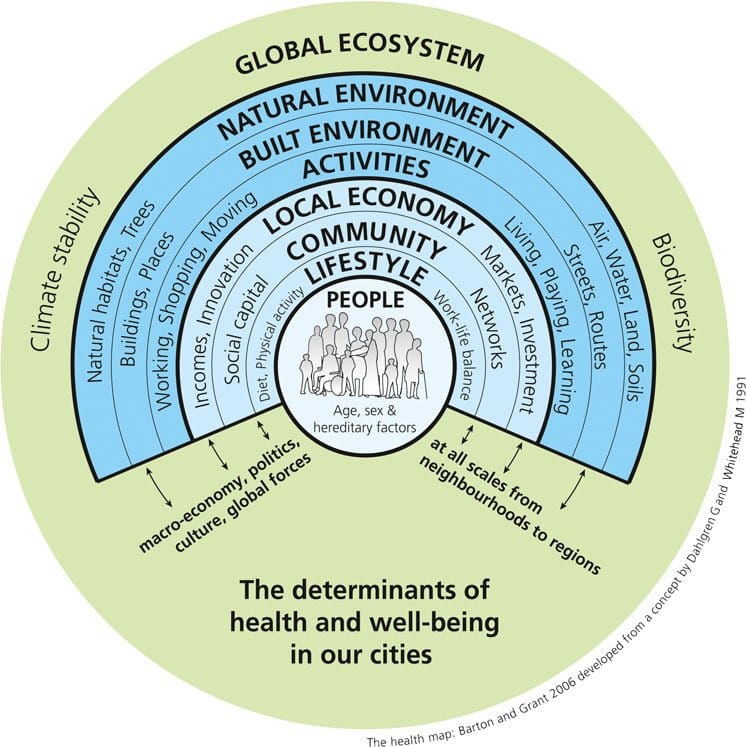
Freeston and Wheeler (2015), in outlining the history of urban planning “through the lens” of public health in the mid-19th century, note how the attention that medicine, psychology and sociology have gradually placed on environmental conditions as decisive factors for health has led to the expansion and development of this field of study, but it has also produced a discontinuous relationship between urban planning and the planning of public health. Corburn (2015) also supports the current separation between urban design and health sciences. To overcome this, Barton and Grant (Barton et al. 2015) propose a framework: “The Settlement Health Map” (fig. 2).
So some questions should be raised: what role does design play, if it still plays a role, in the creation of healthy spaces? Which disciplinary and professional contributions is it required to make?
The question of the role of design refers to the contemporary work of urban planners and architects experiencing conditions of complexity and uncertainty, influence from political and market interests, and legal and financial restrictions. All this often requires the designer to play the role of interpreter and coordinator, which is anything but irrelevant to the success of the project. The health-conscious architect must then, in collaboration with other disciplines and operators, make use of technical-procedural instruments capable of highlighting the health implications of the design choices and keeping them under control, exemplifying and discussing good practices, examining the feasibility and management of the interventions and demanding verifications and evaluations of the results (Barton et al. 2000, 2017; CABE 2009; Capolongo et al. 2015, 2016; Caprotti et al. 2017; Fudge et al. 2003; Lan et al. 2016; Large et al. 2015; Rydin et al. 2012; Talukder et al. 2015). The summary of all this is what Gregotti referred to as “giving meaning to the set of technical choices” (Gregotti 1991), with “meaning” in this case being the health and physical, psychological and social well-being of people in that context, with those requirements and expectations, and in that culture. The health-conscious architect can operate, in synergy with other disciplines and professions, and above all with medical ones, with an Evidence-Based Design logic, namely design based on the results of empirical research, statistical data, investigations, observations and field trials15 (Carmona 2010; de Leeuw et al. 2014; Sallis et al. 2016). We must however observe, as Grant did, that by intervening in the transformation of complex and adaptive systems, such as cities and spatial-social contexts, Evidence-Based Design will not necessarily produce robust results that can be generalised. “Cities can be our laboratories for change, but not if we have to wait 50 years from conclusive dose-response evidence for cycling and walking and health impact of active transport to see a transformation in mainstream city design” (Grant et al. 2017). There is therefore a contribution to be made with research using design methods to find a synthesis between the different skills and the different scientific acquisitions, working on the theme of the relationship between places, the context and health, (Dannenburg et al. 2011; Rydin et al. 2012), and in particular on some topics: public space (Bianchetti 2016; Lauria 2017; Van Hecke et al. 2018; Ward Thompson et al. 2002), the district (Barton et al. 2010; Godhwani 2018; Van Cauwenberg 2016; Valera Sosa 2016), urban green areas (Ward Thompson et al. 2016), parks (Marzi L. et al. 2018), play areas (Lawrence et al. 2003; Mahdjoubi et al. 2015), transport and pedestrian and cycle paths (Davis et al 2015; Nieuwenhuijsen 2018; Sallis et al. 2016), the hospital (Del Nord et al.2006; 2012; Serrazanetti 2017; Setola et al. 2016), and housing (Marco et al. 2015; Perriccioli 2015) .
Exemplary projects
Peter Hall, in his latest book, mentions Copenhagen as one of the most attractive capitals. “small and welcoming, it is a city where people rather than cars set the pace, with a multitude of pedestrianazed thoroughfares, green spaces and cycle lines […] one of the most ‘liveable’ cities on the planet.” (Hall, 2014, p.232) and this is thanks to research on the design of public spaces conducted by Danish architects starting with Jan Gehl (Gehl, 2008) through to the COBE Architects17
It is once again Peter Hall, in “Good Cities, Better Lives,” who says that Freiburg is “The city that does it all,” and Grant and Burton mention it in their book (2017, p. 540) saying that not only is there a quality urban environment and a good social atmosphere, but “the principles of healthy urban planning were here made visible, and they worked.” Since the Seventies the urban redesign of Freiburg has represented an example of the integration of environmental and social principles, sustainable mobility and limitations on the land use, with clear objectives pursued in a firm way, involving the community, private and public operators and the university. (fig. 4)
At building scale, the redevelopment and construction of the new Meyer Children's Hospital in Florence (Donati 2007) is one of the most award-winning and mentioned examples of European hospitals that are person centered and environmentally friendly. In this highly specialized children’s hospital, effective treatment is also promoted through the environmental and innovative design of the interior and exterior spaces, from the perspective of Healthy Hospital Healthy Planet and in line with the hilly landscape and the historical park surrounding the complex. (fig. 5)
The examples mentioned are evidence of the importance of integration among all these aspects in the design of spaces for health and lead us to observe how little, at least in Italy, is invested in these topics in university education in architecture. As Lawrence claims (2017 p. 89), it is a question of promoting the capacity to design by staging an “intentional organisation,” a setting guided by “intentional rationality” no less, aimed at promoting the health and well-being of people in the performance of their activities.
The contribution of Architectural Technology
In the design of health spaces each discipline can make its contribution based on its fundamentals and tools. What specific knowledge and tools can Architectural Technology provide?
Architectural Technology is based, in research and in the profession, on an approach aimed at transferring to the design acquisitions that are anchored in natural and social sciences with an experimental and generalist vision. Architectural Technology has an experimental approach that leads it to make the project aims explicit, to verify their effectiveness and to search for innovative solutions. This approach is consistent with that promoted for Healthy Cities and Healthy Settings. The tools and methods of the technological design of architecture (Frameworks, Briefing, Evidence-Based Design, Critical Design in Alternative Scenarios) are useful to keep the design choices under control in relation to the purposes and to develop methods of verification. The need to coordinate different expertise and knowledge to design cities and buildings for health also finds in architectural technologies methods and tools for managing the design, promoting the digitalization of the design, construction and management process. Beyond the specialist contribution, the contribution of technology must, in my view, manifest in a design culture geared towards the health and well-being of people, developing the capacity for “technological imagination,” a quality that allows the designer to innovate when faced with new or age-old problems, with a vision projected towards the future and change, imagining possible and feasible proposals.
Notes
1. See https://www.healthycitiesbelfast2018.com/scope-and-purpose. [accessed 3 December 2018].
2. Human Health is a "damage category" or "endpoint" impact category in an environmental impact assessment, it is a normalized indicator at a global, regional or local level depending on the character of the analysis and assessment.
3. The Healthy Settings Movement derives from the WHO Strategy of Health for All 1980. This approach was most clearly explained in 1986 in Ottawa with the Charter for Health Promotion. http://www.who.int/healthy_settings/about/en/) [accessed 3 December 2018].
4. “A healthy city is one that is continually creating and improving those physical and social environments and expanding those community resources which enable people to mutually support each other in performing all the functions of life and developing to their maximum potential.” WHO, Health Promotion Glossary(1998).
5. The definition of health is given as a premise of the constitution of the WHO adopted in NY in 1946 and which came into force in April 1948.
6. See http://www.who.int/healthy_settings/types/cities/en/. [accessed 3 December 2018].
7. See (SDGs) 17 Sustainable Development Goalsof the “2030 Agenda for Sustainable Development", which was adopted in 2015 and entered into force in 2016.
8. DALY is a term used in the medical context and it has been introduced into many environmental impact analysis methods. It is an indicator that quantifies the impact in terms of the number of years lost due to disability or premature death.
9. See http://www.euro.who.int/en/health-topics/environment-and-health/urban-health/who-european-healthy-cities-network/membership/list-of-phase-vi-healthy-cities, [accessed 3 December 2018].
10. See the Shanghai Declaration on promoting health in the 2030 Agenda for Sustainable Development 21 November 2016.
11. See Jennifer L. Pehr, Health Care and Infrastructure in Accra, Ghana Advanced Issues in Urban Planning 27 April 2010, http://mci.ei.columbia.edu/files/2013/03/Health-Care-and-Infrastructure-in-Accra-Ghana.pdf [accessed 3 December 2018].
12. See http://www.worldbank.org/en/news/feature/2014/01/29/welcome-to-the-healthy-villages-in-china [accessed 3 December 2018].
13. See http://www.arpat.toscana.it/notizie/arpatnews/2015/134-15/134-15-lo-studio-dell-oms-sulle-condizioni-dell-ambiente-indoor-a-scuola. [accessed 3 December 2018].
14. see https://www.who.int/healthy_settings/types/schools/en/ [accessed 3 December 2018].
15. Since the 1990s, public health research has adopted the Evidence-Based methodology (based on experimental research with proof of evidence) using more or less robust and generalizable approaches. This methodology, typical of interdisciplinary research, in particular in the field of medical and social sciences, was also transferred to design research in relation to health, within the framework of methods of verifying the effectiveness of the design in relation to the purposes.
16. The Kuopio model was also developed with the contribution of researchers from Aalto University Centre for Urban and Regional Studies (YTK) and the Finnish Environment Institute (SYKE), and the planners of eight cities and three regions in Finland, see Trading Between Land Use and Transportation Planning: The Kuopio Model available from: https://www.researchgate.net/publication/299807901_Trading_Between_Land_Use_and_Transportation_Planning_The_Kuopio_Model/figures?lo=1&utm_source=google&utm_medium=organic [accessed 3 December 2018].
17. See http://www.cobe.dk/project/our-urban-living-room#3215 [accessed 3 December 2018].
Bibliographical references
Angelucci F., Cellucci C. (2016), “Il paradigma della healthy city tra permanenze e innovazioni nelle piccole città. Prospettive tecnologiche per il sistema degli spazi urbani aperti”, in Techne n.12, 2016, pp. 129-136, FUP, Firenze, IT.
Barca F., Casavola P., Lucatelli S. (2014) Strategia nazionale per le aree interne: definizione, obiettivi, strumenti e governance, Materiali UVAL, n.31, 2014 http://www.dps.gov.it/it/pubblicazioni_dps/materiali_uval.
Barton H., Grant M. (2006) “A health map for the local human habitat.” The Journal for the Royal Society for the Promotion of Health, 126 (6). pp. 252-253. ISSN 1466-4240
Barton H., Tsourou C. (2000), Healthy urban planning in practice: experience of European cities Report of the WHO City Action Group on Healthy Urban Planning. Taylor & Francis.
Barton H., Thompson S., Burgess S., Grant M. (eds.) (2015), The Routledge Handbook of Planning for Health and Well-Being, pp.37-47, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Barton H. (2017), City of Well-Being: A Radical Guide to Planning, Oxford, Routledge, UK.
Barton H., Grant M., Guise, R. (2010), Shaping neighbourhoods: for local health and global sustainability. 2nd ed. Oxford: Routledge. UK.
Bellaviti P. (2005), Una città in salute. Healthy Urban Planning a Milano: un approccio e un programma per una città più sana, vivibile, ospitale. FrancoAngeli, 2005.
Bianchetti C. (2016) Spazi che contano. Il progetto urbanistico in epoca neo-liberale, Donzelli, Roma, IT.
Botchwey D., Hobson S.E., Dannenberg A.L., Mumford K.G., Contant C.K., McMillan T.E., Jackson R.J., Lopez R., Winkle C. (2009), “A Model Curriculum for a Course on the Built Environment and Public Health: Training for an Interdisciplinary Workforce”, American Journal of Preventive Medicine, Vol. 36, Issue 2, Supplement, 2009, pp. S63-S71.
Buffoli M. (2014), Urban Health: strategie per la sostenibilità urbana, FrancoAngeli, Milano, IT.
CABE (2009), Future health: sustainable places for health and wellbeing, CABE, London, UK.
Carmona M.,Gallemt N., Sarka R. (2010), Housing standards : evidence and research. Space standards: the benefit, University college London for Cabe, London, UK.
Capolongo S., Buffoli M., Oppio A. (2015), “How to assess the effects of urban plans on environment and health” in Territorio n°2/2015.
Capolongo S., Buffoli M., Rebecchi A., Di Gregori V. (2015), “Attività fisica quale strategia per la promozione della salute urbana” in Sistema Salute, 2015 Apr-Giu:59(2), pp. 220-227.
Capolongo S., Buffoli M. (2004), “Il contesto urbano: strutture e infrastrutture, le città attive”, in Il guadagno di salute attraverso la promozione dell’attività fisica evidenze scientifiche e attività di campo. Liguori G. Editore.
Capolongo S. (2009), Qualità Urbana, stili di vita, salute: indicazioni progettuali per il benessere. Milano: HOEPLI.
Capolongo S., Lemaire N., Oppio A., Buffoli M., Gall A., Roue L. (2016), “Action planning for healthy cities: the role of multi-criteria analysis, developed in Italy and France, for assessing health performances in land-use plans and urban development projects” in Epidemiologia e Prevenzione, vol.40, fasc. 3-4, pp. 257-264.
Caprotti F. et al. (2017), “The new urban agenda: key opportunities and challenges for policy and practice”, in Urban research & practice, pp.1–12.
Corburn J. (2015), “Urban inequities, population health and spatial planning”, in The Routledge Handbook of Planning for Health and Well-Being, pp.37-47, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Dahlgren G., Whitehead M. (1991). "The main determinants of health" model, version accessible in: Dahlgren G, and Whitehead M. (2007) European strategies for tackling social inequities in health: Levelling up Part 2. Copenhagen: WHO Regional Office for Europe http://www.euro.who.int/__data/assets/pdf_file/0018/103824/E89384.pdf.
D’Alessandro D., Buffoli M., Capasso L., Capolongo S., Fara G.M., Rebecchi A. (2015), “Green area and public health: improving wellbeing and physical activity in urban context”, in Epidemiol Prev. 2015, JuAug. 39(4) suppl 1, pp. 8-13.
Dannenburg H., Jackson R.J. (eds) (2011), Making healthy places IslandPress, Washington DC, USA.
Davis A., Parkin J. (2015), “ Active travel: its fall and rise”, in The Routledge Handbook of Planning for Health and Well-Being, pp.37-47, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
De Leeuw E. (2001), “Global and local (glocal) health: the WHO healthy cities programme”, in Global Change & Human Health, Volume 2, No. 1 (2001), Kluwer Academic Publishers, pp.34-45.
De Leeuw E., Tsouros A., Dyakova M., Green G. (2014), Healthy cities Promoting health and equity - evidence for local policy and practice. Summary evaluation of Phase V of the WHO European Healthy Cities Network. Copenhagen Denmark, WHO; 2014.
Del Nord R. (ed.) (2006), Lo stress ambientale nel progetto dell’ospedale pediatrico. Indirizzi tecnici e suggestioni architettoniche, Motta, Milano, IT.
Del Nord R., Peretti G. (ed.) (2012). L’umanizzazione degli spazi di cura. Linee guida, Ministero della Salute TESIS, Firenze, IT.
Donati C. (2007), “Polo Pediatrico Meyer di Careggi, Firenze, 2000-2007”, in CSPE Centro Studi Progettazione Edilizia. L’innovazione tecnologica dalla ricerca alla realizzazione, Electa, Milano, IT.
Freeston R., Wheeler A. (2015), “Integration health into town planning: a history”, in The Routledge Handbook of Planning for Health and Well-Being, pp.17-36, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Fudge C., Fawkes S. (2018), “Science meets imagination – cities and health in the twenty-first century”, in Cities & Health, vol. 1 issue 2, pp. 101-106.
Fudge, C. (2003), “Health and sustainability gains from urban regeneration and development”. In: T. Takano, (ed.), Healthy cities and urban policy research. London, Routledge, 41–58.
Gehl J. (2010), Cities for people, Island Press, Washington, Covelo, London, USA/UK.
Gehl, J. (1987), Life Between Building, Danish Architectural Press, Copenhagen, DK.
Godhwani S., Jivraj S., Marshall A., Bécares L. (2018), “Comparing subjective and objective neighbourhood deprivation and their association with health over time among older adults in England”, in Health & Place, 2018, ISSN 1353-8292.
Grant M. et al. (2017), “Cities and health: an evolving global conversation” in Cities & Health, vol. 1, 2017 issue 1, pp.1-9.
Gregotti V. (1991), Dentro l’architettura, Bollati Boringhieri, Torino, IT.
Hall P. (2014), Good Cities, Better Lives. How Europe discovered the lost art of urbanism, Routledge, Taylor and Francis group. London New York, UK USA.
Hancock T., Duhl, L. (1986), Healthy cities: Promoting health in the urban context, WHO Regional Office Europe, Copenhagen.
Howard G., Blogh C., Goldstein G., Morgan J., Prüss-Üstün, A. et al. (2002), Healthy villages: a guide for communities and community health workers , Geneva: World Health Organization
http://www.who.int/iris/handle/10665/42456.
Konsonen L. (2015), “The three fabrics strategy in Finland”, in The Routledge Handbook of Planning for Health and Well-Being, pp.74-84, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Lan W. Ross C. (2016), “Healthy City Planning and Assessment: Initiation and Trend”, in UPI Planning D, doi: 10.22217/upi.2016.326.
Large M., Barton H. (2015), “Community housing and place making: narratives, forms and process for convivial living”, in The Routledge Handbook of Planning for Health and Well-Being, pp.37-47, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Lauria A. (a cura di) (2017) . Piccoli Spazi Urbani. Valorizzazione degli spazi residuali in contesti storici e qualità sociale, pp. 59-75, Liguori, Napoli IT.
Lawrence D.F.,Engelke P.O., Schmidt T.L. (2003), Health and Community Design. The impact of the built environment on physical activity. Island Press, Washington, Covelo, London, USA, UK
Lawrence R.J. (2015), “Mind the gap: bridging the divide between knowledge, policy and practice”, in The Routledge Handbook of Planning for Health and Well-Being, pp.74-84, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Mahdjoubi L., Spencer B.(2015), “Healthy play for all ages in public open spaces”, in The Routledge Handbook of Planning for Health and Well-Being, pp.74-84, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Marco E., Burgess S. (2015) “Healthy Housing”, in The Routledge Handbook of Planning for Health and Well-Being, pp.74-84, Routledge Taylor & Francis, Oxfordshire, UK, New York, USA.
Marzi L., Setola N., Torricelli M. C. (2018), “Accessibility indicator for a trails network in a Nature Park as part of the environmental assessment framework”, Environmental Impact Assessment Review, vol. 69, pp. 1-15.
Nieuwenhuijsen M., Khreis H. (ed.) (2018), Integrating Human health in Urban and Transport Planning. A Framework, Springer Int. Pub.
Perriccioli M. (ed.) (2015), RE-Cycling Social Housing Ricerche per la rigenerazione sostenibile dell’edilizia residenziale sociale, CLEAN, Napoli, IT.
Rydin Y., Bleahu A., Davies M., Dávila J.D., Friel S., De Grandis G., Groce N., Hallal P.C., Hamilton I., Howden-Chapman P., Lai K.M., Lim C.J., Martins J.,
Osrin D., Ridley I., Scott I., Taylor M., Wilkinson P., Wilson J. (2012), “Shaping cities for health: complexity and the planning of urban environments”, in The 21st century. Lancet. 2012 Jun 2, 379(9831), pp. 2079-108.
Sallis J. F., Bull F., Burdett R., Frank L. D., Griffiths P., Corti B. J., Stevenson M. (2016), “Use of science to guide city planning policy and practice: how to achieve healthy and sustainable future cities”, The Lancet, Volume 388, Issue 10062, 2016, pp. 2936-2947.
Serrazanetti F. (ed.) (2017), TAMassociati. Taking care. Architetture con Emergency, Mondadori Electa. Milano. IT.
Setola N., Borgianni S. (2016), Designing Public Spaces in Hospitals, Routledge - Taylor and Francis Inc., New York and Abingdon, Oxon, USA.
Stewart-Brown S. (2006), What is the evidence on school health promotion in improving health or preventing disease and, specifically, what is the effectiveness of the health promoting schools approach? Copenhagen, WHO Regional Office for Europe (Health Evidence Network report; http://www.euro.who.int/ document/e88185.pdf, (accessed 01 March 2006).
Talukder S., Capon A., Nath D., Kolb A., Jahan S., Boufford J. (2015) Urban health in the post-2015 agenda. Lancet. 2015 Feb 28, 385(9970):769.
Valera Sosa A. (2017), “Medical Neighbourhoods: Urban Planning and Design Considerations for Charité Virchow Klinikum in Berlin, Germany”, in
Mathiasen N. and Frandsen A.K. (Eds), ARCH 17 3rd international conference on architecture, research, care and health Conference Proceedings, Lars Brorson Fich Polyteknisk forlag. pp.163-186.
Valera Sosa A. (2017), “Medhoods: building neighbourhood health ecosystems”. In Nickl-Weller C., Healing Architecture 2004-2017, Braun. pp.176-179.
Valera Sosa A., Nickl-Weller C. (2016), “Understanding walkability and walking rates in Berlin: an urban form and street pattern comparison”, in Die Psychiatric, 2/2016, pp. 79-87.
Van Cauwenberg J., Van Holle V., De Bourdeaudhuij I., Van Dyck D., Deforche B. (2016) “Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity”,in Health & Place, Volume 37, 2016, pp. 16-25.
Van Hecke L., Ghekiere A., Veitch J. ,Van Dyck D., Van Cauwenberg J., Clarys
P., Deforche B. (2018), “Public open space characteristics influencing adolescents’ use and physical activity: A systematic literature review of qualitative and quantitative studies”, in Health & Place, Volume 51, 2018, pp. 158-173.
Ward Thompson C., Aspinall P., Roe J., Robertson L., Miller D. (2016), “Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment”, Int J Environ Res Public Health. 2016 Apr 22;13(4):440. Published online 2016 Apr 22. doi: 10.3390/ijerph13040440.
Ward Thompson C., Roe J., Aspinall P. (2013), “Woodland improvements in deprived urban communities: what impact do they have on people’s activities and quality of life?”, in Landscape and urban planning, 118, pp.79–89.
Ward Thompson, C. (2002), “Urban open space in the 21st century”, in Landscape and urban planning, 60 (2),59–72.10.1016/S0169-2046(02)00059-2.
WCED, Brundtland Commision (1987), Our Common Future, Oxford University Press, UK.
Whitehead D., (2004), “The European Health Promoting Hospitals (HPH) project: How far on?”, in Health Promotion International. 19(2): 259.
WHO (2002), Healthy Villages: A guide for communities and community health workers, WHO, Geneva, SW.
WHO Regional Office for Europe (2012), Action Plan for implementation of the European Strategy for the Prevention and Control of Noncommunicable Diseases 2012−2016.
WHO Regional Office for Europe (2013), Health 2020: a European policy framework supporting action across government and society for health and well-being.
WHO (2018), Housing and health guidelines. https://www.who.int/sustainable-development/publications/housing-health-guidelines/en/.
Wilburn S., Karliner J. (ed.), WHO’s Department of Public Health and Environment and Health Care Without Harm (2009), Healthy hospitals, healthy planet, healthy people: Addressing climate change in healthcare settings.WHO HCWH, report http://www.who.int/globalchange/publications/climatefootprint_report.pdf?ua=1, (accessed 30 Nov. 2018).
Williams A. (2017), China’s urban revolution. Understanding Chinese eco-cities, Bloomsbury Academic, Londra, UK, NY, USA.
Williams A. (2018), “China’s shift from urban development to rural reconstruction”, in Architectural Review, April, EMAP Publishing Limited, UK.
Xiaodong T., Xiangxiang L., Haiyan S. (2017), “Healthy China 2030: A Vision for Health Care”, in Value in Health Regional Issues 12C (2017) 112 – 114.c


EWT/ EcoWebTown n.18
Journal of Sustainable Design | Rivista semestrale on line - Online Six-monthly Journal
Edizione Spin Off SUT, Sustainable Urban Transformation, Università Chieti-Pescara
ISSN 2039-2656 Registrazione Tribunale di Pescara n° 9/2011 del 07/04/2011